




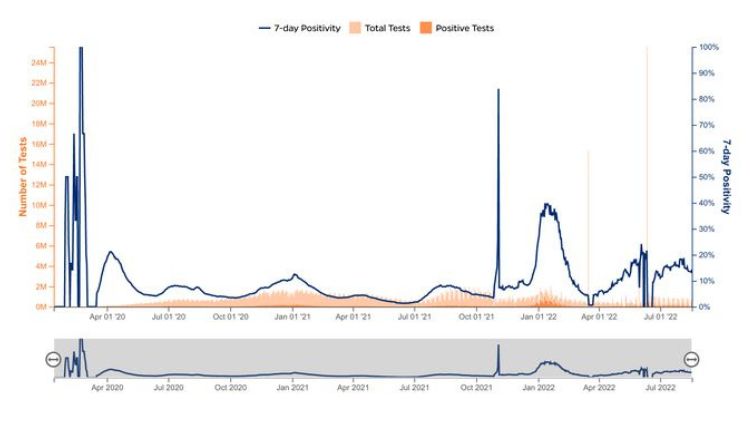
The change in data collection that started on March 3 when the Coronavirus Resource Center (CRC) started getting data from the Johns Hopkins Centers for Civic Impact instead of the COVID Tracking Project (CTP), which ceased operations on March 7, was the cause of previous spikes in historical data for total and positive tests in the graphic. Additionally, non-resident testing in Florida and Alaska as well as probable cases in Hawaii are now included in the CRC.
In order to assess the COVID-19 infection rate in the United States and determine whether enough testing is taking place, it is crucial to monitor the testing that states perform to identify people who have the illness. The number of viral tests conducted and the number of patients for whom they were conducted should be included in the number of COVID-19 tests that states report. States may not currently be discriminating between the total number of tests administered and the total number of people who have been tested. States should seek to remedy this significant gap in the data that is currently available to track testing in the United States.
States should not include serology or antibody tests when reporting COVID-19 infection testing numbers. Antibody tests are not utilised to identify an active COVID-19 infection, and they do not reveal the number of COVID-19 cases that have been identified or whether viral testing is enough to identify infections that are present in each state. States that count serology tests as part of their total COVID-19 testing counts are overstating their testing capabilities and their degree of community-wide COVID-19 infection detection efforts. States that want to track the quantity of serology tests run should publish those figures separately from the quantity of viral tests run to identify COVID-19.
dailyusamail






